Poison in the Air: The 1890 Influenza Pandemic in Singapore
The 1890 influenza pandemic – which a medical official called a “poison” arriving from the ships – was Singapore’s first major outbreak. From the wharf, the pandemic spread quickly to hospitals, houses, and schools, and it affected all social groups. A public memory of the outbreak survived in the aftermath sustained by newspaper articles and the promises of miracle cures. The 1890 pandemic provides interesting comparisons with the COVID-19 outbreak in Singapore, while also sounding a note of caution on the lessons we may draw from history.
The 1890 pandemic was Singapore’s first recorded influenza outbreak. It reportedly “prevailed almost everywhere,” 1 yet historians know virtually nothing about it. In the aftermath of the pandemic, falling ill with influenza was not an uncommon experience. For sufferers, the illness imbued familiar everyday objects with new and unpleasant meanings. It also left a deep imprint on people’s memories.
We place these social experiences and memories in context by tracing the history of the pandemic, from its origins and spread to its aftermath. This offers us a new perspective on Singapore’s response to the ongoing COVID-19 pandemic. The differences between the two outbreaks are obvious, but less so are the “lessons,” if any, that we can learn from the 1890 crisis.
Arrival at the wharf
The 1890 influenza pandemic arrived in Singapore in the third week of February and lasted until the start of April before disappearing quite abruptly – a duration of six to seven weeks. The quarantine system on St John’s Island, which inspected inbound ships for signs of infectious disease, was undeveloped and undermanned at the time. It did not take precautions to thwart the entry of influenza into Singapore. The bulk of quarantine work during the year took place between September and December, mainly to quarantine sea passengers suffering from cholera and smallpox. 2
During the pandemic, the Acting Principal Civil Medical Officer wrote in his report to the Colonial Office: “In Singapore I am of the opinion that the disease was introduced by ships, probably by the wharf coolies being infected by contact with persons on board ships suffering from the disease, or working in the air of ships that had become charged with the Influenza poison.” 3 The report was submitted to the Colonial Office nearly half a year later. It described the illness as characterised by high fever (up to 40 degrees Celsius), severe headaches, back and muscular pains, and intense bouts of coughing, with some patients describing how their heads were “splitting open.”
Singapore then became the conduit for the spread of influenza to Penang (where the first case was reported in the first week of March) and Malacca (the first week of April). Unlike in Penang, where the outbreak was traced to coolies opening cases of piece goods in the local bazaar, the Acting Principal Civil Medical Officer pinpointed the Singapore outbreak to have occurred among the wharf workers. Singapore’s was an unsurprisingly severe outbreak, as the coolies “live together in a large building in a very overcrowded condition.” 4
The Straits government did not make influenza a notifiable disease, as was done during the 1918 influenza pandemic. It did not release the complete official numbers of cases and deaths, though there were some statistics on the monthly death rate. Both the government and the Municipal Commission stated that the number of direct deaths from influenza was very small, though the complications that resulted were more serious. The Acting Principal Civil Medical Officer estimated the death rate to be no more than 0.5 percent, due to the “attenuated condition” of the imported virus; when it occurred, death was due to pneumonia or the poor health of debilitated coolies. 5
The Municipal Commission, which oversaw the administration of the town, added that most fatalities were old people or others suffering from “cardiac or pulmonary affections,” adding, “Although not of itself a fatal disease, yet its influence in increasing the death rate during an epidemic is remarkable.” 6 Unfortunately, we have little information on the complications, too, other than the figures of 800 admissions and 150 deaths due to respiratory illnesses in the Straits Settlements that year.
We do have the Registrar-General’s submission that the greatest number of monthly deaths in in that year occurred in March. In most years, this was apparently among Singapore’s healthiest months, but in 1890, there were 661 deaths at the height of the influenza pandemic. The corresponding mortality figures for February and April 1890 were 420 and 598, respectively, with a monthly average of 546 for the year. 7 This suggests that, conservatively, influenza was responsible for about 120 deaths.
To hospitals and schools
The colonial records tell us little about the spread and trajectory of the pandemic in Singapore as a whole. Medical reports continued to focus on the zymotic illnesses the government had long tracked: bubonic plague, cholera, and smallpox. The exception was the government hospital records, which were the few official sources of information on an acute disease that broke out and ended suddenly. The government did not possess records on how or how far influenza was spreading in the community. On the other hand, hospital records must be regarded with scepticism, for many people did not seek treatment in hospitals, which also did not prevent the outbreak from spreading quickly into the population.
In the General Hospital (GH), two cases of influenza were admitted to the European wards during the year; both subsequently recovered. Four cases were admitted to the Native (Asian) wards, who also recovered. As these were small numbers, we can infer they were the severe cases, whereas most patients suffering from a mild infection did not seek help at the hospital. By contrast, there were 46 cases of mild influenza admitted to the Police ward of the GH. In addition, the hospital noted, “the bulk of the cases of bronchitis, febricula (a mild fever) and rheumatism were admitted at or about the time of the prevalence of influenza.” 8
The strongest evidence of uncontrolled spread was the large increase in the number of total admissions to the Prison Hospital, from 695 in 1889 to 1000 in 1890, with the first admission made on 8 March. The actual number attributed to influenza was only 136, mostly during this month; among them were six Europeans. Three patients later died from pneumonia caused by influenza, including an English soldier. These admissions to the Prison Hospital were only the tip of the iceberg, with half of the 1000 prison inmates reportedly suffering from influenza that year. The prison authorities reported that “hundreds of slighter cases were treated among the prisoners in the prison, the patients being put on light work.” 9 In general, the prison hospital did not admit sick prisoners unless their illness prevented them from working.
Infections were also reported in the hospital for women’s sexually transmitted diseases and in outdoor dispensaries, suggesting the spread of the disease into the surrounding municipal area. Surprisingly, the Tan Tock Seng Hospital (TTSH), a major hospital originally built for Asian paupers in Singapore, treated a mere four cases of influenza. It claimed to have avoided an outbreak of influenza among its patients, but this seems doubtful.
As the disease was not made notifiable, it was difficult to prevent the spread of infection to the general population. We do not know exactly how the “poison” spread beyond the wharves, as the colonial and municipal records are patchy on the matter. The Acting Principal Civil Medical Officer felt that women were less affected than their husbands, as they resided in well-ventilated homes most of the time, though this would not apply to women who did not dwell in such good homes or those of lesser means. Working-class Asian women in the town typically lived in shophouses, which had poor air circulation, or wooden houses.
But the spread of influenza inside the Prison Hospital suggests that there was little resistance to its penetration into an unprepared general population. On 8 March, the Straits Times reported that “there is scarcely a Chinese house in the district of Teluk Ayer street where one or more is not suffering from the disease,” 10 including a Chinese Municipal Commissioner, his family, and servants. This charts a path of infection from the wharves to the streets of densely-populated Chinatown within walking distance, where the coolies lived. Three days later, the newspaper deemed that “Influenza seems to be getting still more prevalent in Singapore, especially among the Asiatics.” 11
The paper carried a lengthy report on the same day, criticising the “woful [sic] ignorance” of even the educated public. The report surmised that the pandemic was spreading unevenly among the social classes and ethnic groups of the municipal population, with poorer and Asian groups being more heavily affected: “So far the malady has made only modest headway among the European or Eurasian population, and is most prevalent among the Chinese, Tamils and some of the poorer classes of Portuguese residents […] whereas at Tanjong Pagar [near the busy port area], numbers of the wharf coolies are much affected by it.” 12 However, the article also found increased absences of pupils in Singapore’s leading schools. This provided an insight into influenza’s movement across different demographics – among students and within their families. At the Tamil School at Cross Street, some staff and as many as half the students were absent due to “bona fide influenza.” St. Anthony’s Mission School seemingly “got it bad” as well, reporting a similar proportion of student absentees. By contrast, in the Anglo Chinese School, only a fifth of the boys were absent from class, alongside a quarter of the boys at the mission house. At the other extreme, schools such as Raffles Institution Girls School, Raffles Boys School, and St. Joseph’s Institution reported no outbreaks, showing the unevenness of experience (or lack of reliable data) across Singapore. Thus influenza also spread to the upper echelons of Singapore society, as it was mostly the better-educated and higher-income residents who had children and were able to send them to good schools. The bulk of the immigrant Asian population was single or had no children.
Another report in the Straits Times traced the outbreak earlier to late January, with allegedly over 200 influenza cases occurring across all the ethnic groups. It alluded to under-reporting of the outbreak, with a large number of patients not seen by Western-trained doctors but by “the native so-called doctors.” 13 Some patients among the latter group (or those who self-medicated) used an herbal remedy called Kroma susu (possibly a drink, as susu is milk in Malay). This was allegedly “a common weed” commonly used for treating influenza and asthma.
For a sufferer inclined towards Western medicine, a London-based company called F. Comar & Son advertised the product Aubergier’s Syrup and Paste, as a “world-famed and marvellous medicament” for influenza and other respiratory afflictions. 14 Chamberlain’s Cough Remedy remained popular in Singapore as a treatment for “coughs, colds, croup, whooping cough and influenza” into the new century. 15 So did Dr. Williams’ “pink pills for pale people,” sold as a “cure-all” for a princely sum of eight dollars for half a dozen bottles. 16 It was still in use at the time of the 1918 influenza pandemic and thereafter.
The appearance of these commercial products, often replete with glowing testimonials from “consumers,” takes us into the realm of social history and memory. They showed an awareness of influenza and the persistence of fear in the community. During the pandemic, a writer to the Straits Times, with the moniker “A Stitch in Time Saves Nine,” was worried that the influenza would be followed by a cholera outbreak, which allegedly had happened in previous influenza epidemics. 17 Sustained in part by personal concerns and in part by commercial motives, a strand of social memory survived the pandemic. This differed from the official stance in the years after the outbreak.
Aftermath: inactivity and memory
As soon as the pandemic diminished, the 1890 outbreak was virtually forgotten by the government. The medical reports of the Straits Settlements noted sporadic cases of influenza in the ensuing decades, but there were no major plans to deal with a disease that had become endemic. Once again, our main source of information from the colonial government is the medical establishment. In 1891, two cases of influenza were treated in the GH. Two years later, the Straits Times stated that “Whole families have been stricken” by a mild strain of local influenza, though this was something the government failed to report. 18
This happened again in 1895, with outbreaks occurring in England, Spain, and Singapore. The Singapore outbreak was purportedly a severe one, affecting the various ethnic groups; complications were not uncommon. The Straits Registrar-General claimed that there was no outbreak of epidemic disease to explain the year’s relatively high death rate. But a letter to the press by “L.” noted that “The influenza epidemic is right among us,” striking down “Many heads of department.” 19 The disease, the author said, “is no respector of persons.”
Finally, in the middle of 1897, between the months of June and September, the colonial administration reported a mild but fairly large outbreak of influenza. This transpired among the police force, with 443 patients seen at its outpatient department, with many personnel visiting the department two or three times each. This was a prevalent outbreak, affecting policemen from all stations but especially those from the Orchard Road and Kandang Kerbau stations within the town area. It was also a mild outbreak, with few reports of complications except for slight bronchitis and pain in the limbs for several days. Only four patients had to be sent to a hospital, requiring only “a few days in barracks” for a full recovery. 20 The quarantine station on St John did not report any influenza that year.
In the following year, another mild outbreak took place in the Prison Hospital, resulting in 73 cases in March and April. There were no further official reports of influenza events until 1908, when one patient was admitted to the European ward and three were admitted to the Native ward of the GH. The next influenza outbreak was the global pandemic of 1918, which also struck Singapore. There were sporadic deaths from influenza in this period: in 1905, a young Chinese male between 25 and 35; in 1914, a Chinese male above 55; and in 1915, a Malay male.
The 1890 pandemic did not nudge the Straits government nor the Municipal Commission to change their policy on infectious disease. Neither side was keen to take charge of the control of epidemic disease in the town area. In 1894, after a long-running debate with the colonial government, the Commission became the main authority responsible for the control of epidemic disease in the Municipality. One of the pressing issues was to enforce the notification system, as people frequently did not report cases of dangerous infectious disease to the authorities.
But the following year, the President of the Commission Alex Gentle argued against reforming the system: “Singapore has suffered very little from epidemics of recent years, and to establish an elaborate and costly system of espionage in the hope of the early detection of cases of disease, is…uncalled for and might prove mischievous as tending to alienate an Asiatic population from European methods and to confirm them in their habits of secrecy and distrust.” 21 Gentle’s statement is remarkable in two ways: he not only depicted effective notification to be a form of “espionage” that harmed the relationship between the rulers and the ruled, but also ignored the significance of the influenza pandemic just five years earlier. Influenza had not been made a notifiable disease in 1890, allowing it to spread widely among the classes and ethnic groups of Singapore. The Municipal Commission’s stance on notification would have repercussions for Singapore’s response to the 1918 influenza pandemic, when influenza was made a notifiable disease in the Straits Settlements.
Lessons of history?
The 1890 outbreak offers some interesting insights into the ongoing COVID-19 pandemic 130 years later. The differences between these two events are plain to see. Unlike the Singapore government’s robust policy in the current crisis, the colonial response was virtually non-existent. In 1890, the infection spread quickly beyond the wharf coolies to the community, with the hospitals unable to stem the spread. The pandemic affected all social classes, ethnic, and age groups, albeit unequally. Such was symptomatic of a busy entrepôt port that did not halt its business and social activities. This, in turn, reflected the economic priorities of the colonial government and the role of Singapore as an entrepôt.
By contrast, the present government has responded to the COVID-19 pandemic in more purposeful ways. It has calibrated the degree of social distancing and range of public health restrictions in response to evolving circumstances. Nevertheless, at the time of writing (December 2021), Singapore continues to probe a way out of the pandemic after nearly two years of restrictions. It is still premature to conclude that the current response has singularly been more successful. Perhaps the better question to ask concerns the balance of public health and socio-economic costs of the response.
The 1890 pandemic was also quickly forgotten by the Straits government. Even when the global influenza outbreak reached Singapore in 1918, the colonial government did not refer to the earlier event. By contrast, in the current pandemic, the present government initially used the 2003 SARS outbreak as a frame of reference for its response. Influenza did not change colonial policy on epidemic disease either. The status quo prevailed, including the ineffective notification system. As David Arnold notes in the case of India, it is difficult to draw lessons from history when the 1918 influenza outbreak produced little noteworthy change there. 22 Yet, people in Singapore did not forget the “poison” of 1890. As the newspapers continued to carry reports (and advertisements) on influenza, they helped keep the subject alive in locals’ minds. The “lesson” from Singapore, then, might be that social memory is an important part of public health in shaping people’s attitudes and behaviour during influenza outbreaks. 23
Kah Seng Loh is a historian and director of a research consultancy. He is the author of Squatters into Citizens: The 1961 Bukit Ho Swee Fire and the Making of Modern Singapore; Tuberculosis – The Singapore Experience, 1867–2018; and Theatres of Memory: Industrial Heritage of 20th Century Singapore. Email: lohkahseng@chroniclesresearch.com
Li Yang Hsu is a Singaporean infectious diseases physician who researches drug-resistant infections. He is head of the infectious diseases programme and vice dean of global health at the Saw Swee Hock School of Public Health, National University of Singapore. He is the co-author of Tuberculosis – The Singapore Experience, 1867–2018. Email: mdchly@nus.edu.sg
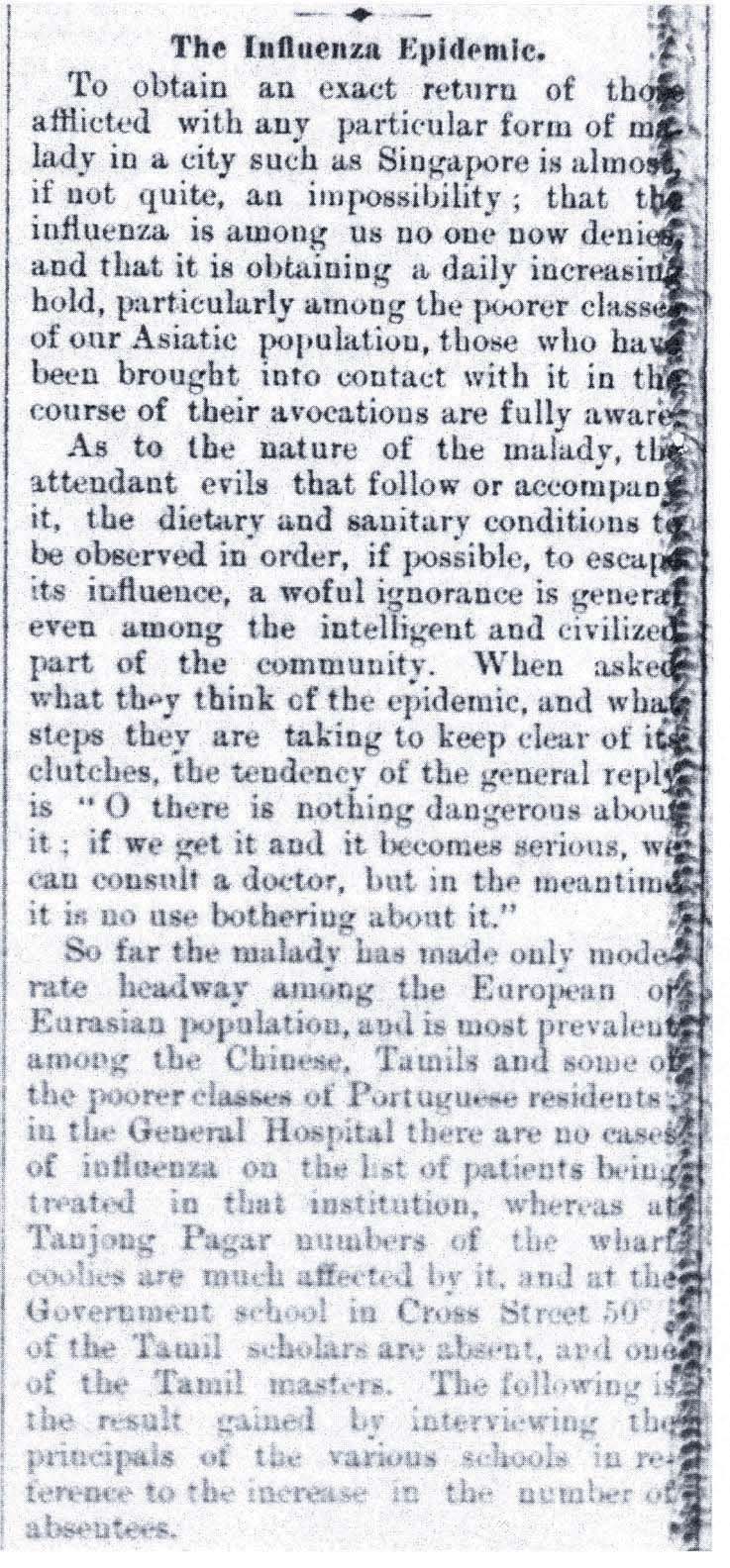
Fig. 1: The Straits Times’ report on the 1890 pandemic, 11 March 1890 (Source: https://eresources.nlb.gov.sg/ newspapers/Digitised/Article/ stweekly18900311-1.2.45).
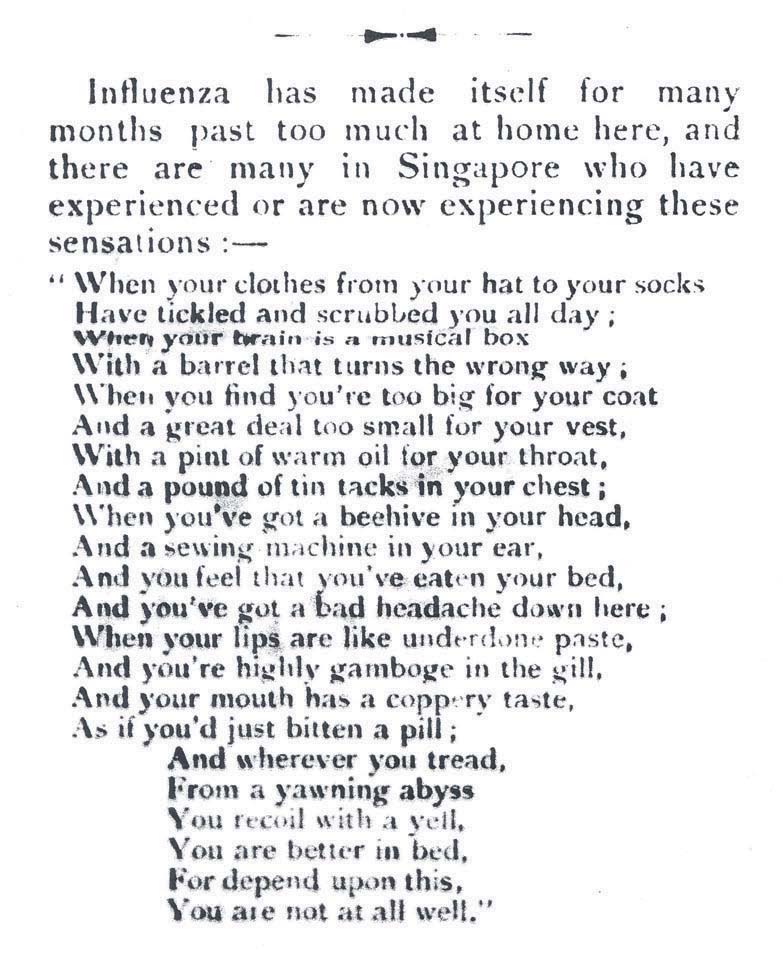
Fig. 2: A poem on being ill with the flu, Singapore Free Press, 5 April 1892 (Source: https://eresources.nlb.gov.sg/ newspapers/Digitised/Article/ singfreepresswk18920405-1.2.14).
Fig. 3: An advertisement for Chamberlain’s Cough Remedy, Singapore Free Press, 22 September 1898 (Source: https://eresources.nlb.gov.sg/ newspapers/Digitised/Article/ singfreepressb18980922-1.2.34).
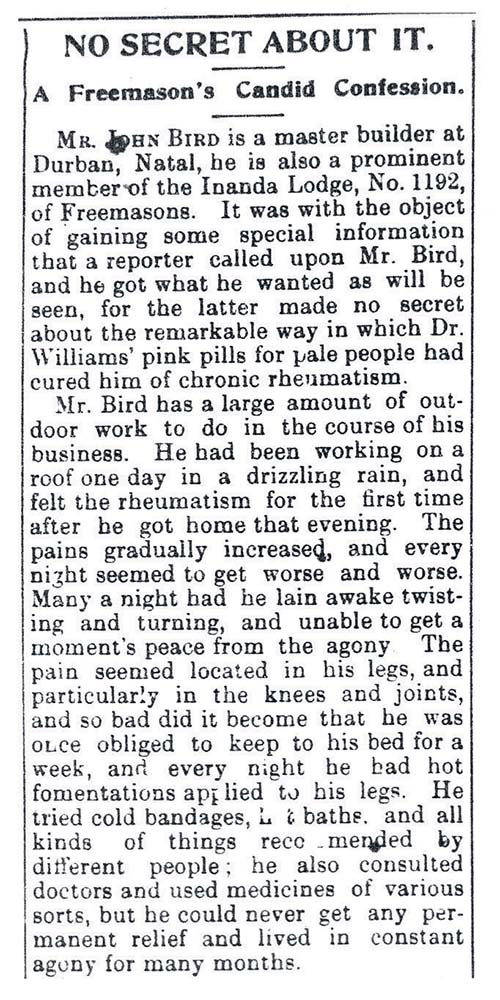
Fig. 4: A “personal account” of the benefits of Dr. Williams’ “pink pills for pale people,” Straits Times, 13 December 1903 (Source: https://eresources.nlb.gov.sg/newspapers/ Digitised/Article/straitstimes19031213-1.2.13).
Fig. 5: A “personal account” of the benefits of Dr. Williams’ “pink pills for pale people,” Straits Times, 13 December 1903 (Source: https://eresources.nlb.gov.sg/newspapers/ Digitised/Article/straitstimes19031213-1.2.13).